8. Available Treatments: the good that’s refused and the bad that is pushed
Summary:
The scientific and medical literature, in addition to our knowledge of COVID-19, clearly indicates the presence of numerous alternative preventative and treatment measures that could be utilized and have been successfully utilized in the treatment of COVID-19. This includes, but is not limited to, anti-inflammatories, anticoagulants, various drugs (e.g. hydroxychloroquine, chloroquine, remdesivir, ivermectin, doxycycline, etc.).
- “In silico studies showed that compounds from propolis [bee glue; a resin-like substance produced by honeybees and used to build hives] could interact with target proteins of SARS-CoV-2, interfering with viral entry and viral RNA replication, while clinical studies revealed that propolis and honey could probably improve clinical COVID-19 symptoms and decrease viral clearance time. However, clinical evidence is limited by the small number of studies and small sample sizes. Future clinical studies are warranted” (Dilokthornsakul et al., 2022)
- “IL-6 [Interleukin-6, a major contributor to the inflammatory processes of COVID-19] induces endothelial dysfunction with TF [Tissue Factor] and CAMs [adhesion molecules] expression via upregulation of ACE2r [primary target of spike protein]. VitD prevented these IL-6 deleterious effects. Thus, it might be speculated that this is one of the hypothetical mechanism(s) by which VitD exerts its beneficial effects in COVID-19 infection.” (Cimmino et al., 2022)
- “Severe acute lung injury has few treatment options and a high mortality rate. Upon injury, neutrophils infiltrate the lungs and form neutrophil extracellular traps (NETs), damaging the lungs and driving an exacerbated immune response. Unfortunately, no drug preventing NET formation has completed clinical development. Here, we report that disulfiram —an FDAapproved drug for alcohol use disorder— dramatically reduced NETs, increased survival, improved blood oxygenation, and reduced lung edema in a transfusion-related acute lung injury (TRALI) mouse model. We then tested whether disulfiram could confer protection in the context of SARS-CoV-2 infection, as NETs are elevated in patients with severe COVID-19. In SARS-CoV-2-infected golden hamsters, disulfiram reduced NETs and perivascular fibrosis in the lungs, and downregulated innate immune and complement/coagulation pathways, suggesting that it could be beneficial for COVID-19 patients. In conclusion, an existing FDA-approved drug can block NET formation and improve disease course in two rodent models of lung injury for which treatment options are limited.” (Adrover et al., 2022)
- “Results: Of the 223,128 citizens of Itajaí considered for the study, a total of 159,561 subjects were included in the analysis: 113,845 (71.3%) regular ivermectin users and 45,716 (23.3%) non-users. Of these, 4,311 ivermectin users were infected, among which 4,197 were from the city of Itajaí (3.7% infection rate), and 3,034 non-users (from Itajaí) were infected (6.6% infection rate), with a 44% reduction in COVID-19 infection rate (risk ratio [RR], 0.56; 95% confidence interval (95% CI), 0.53-0.58; p < 0.0001). Using PSM, two cohorts of 3,034 subjects suffering from COVID-19 infection were compared. The regular use of ivermectin led to a 68% reduction in COVID-19 mortality (25 [0.8%] versus 79 [2.6%] among ivermectin non-users; RR, 0.32; 95% CI, 0.20-0.49; p < 0.0001). When adjusted for residual variables, reduction in mortality rate was 70% (RR, 0.30; 95% CI, 0.19-0.46; p < 0.0001). There was a 56% reduction in hospitalization rate (44 versus 99 hospitalizations among ivermectin users and non-users, respectively; RR, 0.44; 95% CI, 0.31-0.63; p < 0.0001). After adjustment for residual variables, reduction in hospitalization rate was 67% (RR, 0.33; 95% CI, 023-0.66; p < 0.0001). Conclusion: In this large PSM study, regular use of ivermectin as a prophylactic agent was associated with significantly reduced COVID-19 infection, hospitalization, and mortality rates.” (Kerr et al., 2022)
- “While there is no single ‘Silver Bullet’ to cure COVID-19, we believe that the severely disturbed pathological processes leading to respiratory failure in patients with COVID-19 organizing pneumonia will respond to the combination of Methylprednisone, Ascorbic acid, Thiamine, and full anticoagulation with Heparin (MATH+ protocol).We believe that it is no longer ethically acceptable to limit management to ‘supportive care’ alone, in the face of effective, safe, and inexpensive medications that can effectively treat this disease and thereby reduce the risk of complications and death.” (Marik et al., 2021)
- Additionally, the same authors had published a review of “the scientific and clinical rationale behind MATH+ based on published in-vitro, pre-clinical, and clinical data in support of each medicine, with a special emphasis of studies supporting their use in the treatment of patients with viral syndromes and COVID-19 specifically.” (Kory et al., 2021) [NOTE: This article was retracted solely based on a notice received from one of the US hospitals utilizing the MATH+ protocol (Senatra Norfolk General Hospital) which claimed that the data reported in the paper was inaccurate. Problems: The retraction is solely based on claims from a single hospital (no indication of issues with the data from the other hospital (United Memorial Medical Center); ignores the main focus of the paper (the literature review supporting the treatment; reference to the hospital data constitutes ~300 words in a 15-page paper, excluding the citations); ignores the conclusion of the paper which focuses on logic extracted from the literature review and does not address the hospital data. Additionally, there is no indication that the authors were given a chance to respond/correct any issues. The authors claim that they provided the journal with follow-up data, but the journal refused to accept it.]
- Additionally, the same authors had published a review of “the scientific and clinical rationale behind MATH+ based on published in-vitro, pre-clinical, and clinical data in support of each medicine, with a special emphasis of studies supporting their use in the treatment of patients with viral syndromes and COVID-19 specifically.” (Kory et al., 2021) [NOTE: This article was retracted solely based on a notice received from one of the US hospitals utilizing the MATH+ protocol (Senatra Norfolk General Hospital) which claimed that the data reported in the paper was inaccurate. Problems: The retraction is solely based on claims from a single hospital (no indication of issues with the data from the other hospital (United Memorial Medical Center); ignores the main focus of the paper (the literature review supporting the treatment; reference to the hospital data constitutes ~300 words in a 15-page paper, excluding the citations); ignores the conclusion of the paper which focuses on logic extracted from the literature review and does not address the hospital data. Additionally, there is no indication that the authors were given a chance to respond/correct any issues. The authors claim that they provided the journal with follow-up data, but the journal refused to accept it.]
- Tocilizumab (Actemra®)
- is an interleukin-6 (IL-6) antagonist not FDA-approved to treat COVID-19 (if that means anything anymore) i.e., for COVID-19 it is an experimental drug. IL-6 is an inflammatory immune-chemical that is potentially associated with the cytokine storm contributing to COVID-19 (Hojyo et al., 2020;Tang et al., 2020).
- Interestingly, the inflammatory response (including IL-6 levels) to COVID-19 has been reported to be correlated to Vitamin D deficiency (Jain et al., 2020). Tocilizumab is also mentioned, in some other points, in the information below.
- The information on the Medication Guide is noteworthy given what COVID-19 is. It indicates the following warning: “ACTEMRA can cause serious side effects including: 1. Serious Infections. ACTEMRA is a medicine that affects your immune system. ACTEMRA can lower the ability of your immune system to fight infections. Some people have serious infections while taking ACTEMRA, including tuberculosis (TB), and infections caused by bacteria, fungi, or viruses that can spread throughout the body. Some people have died from these infections. Your healthcare provider should test you for TB before starting ACTEMRA.”
- Moreover, the FDA Fact Sheet on tocilizumab, under “Warnings and Precautions” states:
- is an interleukin-6 (IL-6) antagonist not FDA-approved to treat COVID-19 (if that means anything anymore) i.e., for COVID-19 it is an experimental drug. IL-6 is an inflammatory immune-chemical that is potentially associated with the cytokine storm contributing to COVID-19 (Hojyo et al., 2020;Tang et al., 2020).
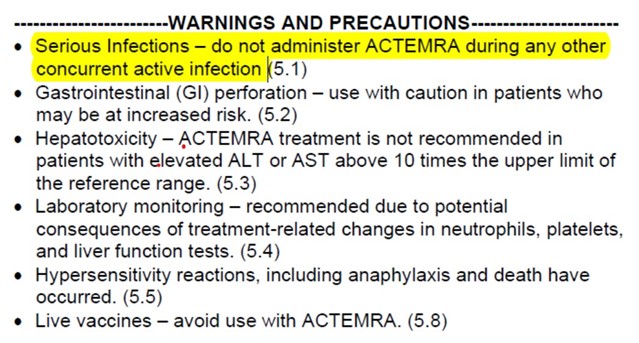
Figure 12: Excerpt from Fact sheet available on FDA website (https://www.fda.gov/media/150321/download)
- Questions for consideration – Given:
- What COVID-19 is (i.e., a viral infection),
- The number of side effects reported thus far with tocilizumab relative to alternate treatments e.g., See McCullough et al. (2020),
- the impact of tocilizumab on the immune-system and increased potential for infections,
does it really make sense to add the potential of increasing infections and lowering immunity to what is already present? Do the benefits really outweigh the risks?
- What COVID-19 is (i.e., a viral infection),

Figure 13: Comparison of reported adverse events: Tocilizumab, Hydroxychloroquine, and Quercetin (http://vigiaccess.org/; data accessed 01//22/22)
- “Virological clearance was earlier in the 5-day ivermectin treatment arm when compared to the placebo group (9.7 days vs 12.7 days; p = 0.02), but this was not the case for the ivermectin + doxycycline arm (11.5 days; p =0.27). There were no severe adverse drug events recorded in the study. A 5-day course of ivermectin was found to be safe and effective in treating adult patients with mild COVID-19.” (Ahmed et al., 2021)
- “Results: The obtained results showed that HCQ [hydroxychloroquine] can inhibit viral replication and entry inside the cell through raising lysosomal pH and binding to specific receptors on the cells, thereby, preventing viral entry. Conclusion: HCQ has a better safety profile than CQ [chloroquine] and also modulates cytokine syndrome.” (Iqbal et al., 2021)
- Preprint stated: “…inhaled budesonide reduced time to recovery by a median of 3 days in people with COVID-19 with risk factors for adverse outcomes” (Yu et al., 2021a) – In the published manuscript in Lancet, this was modified to “Inhaled budesonide improves time to recovery, with a chance of also reducing hospital admissions or deaths” (Yu et al., 2021b)
- Thapsigargin (TG): “Together with its ability to inhibit the different viruses before or during active infection, and with an antiviral duration of at least 48 h post-TG exposure, we propose that TG (or its derivatives) is a promising broad-spectrum inhibitor against SARS-CoV-2, OC43, RSV and influenza virus.” (Al-Beltagi et al., 2021)
- “Administration of the HCQ [hydroxycholorquine] +AZ [azithromycin] combination before COVID-19 complications occur is safe and associated with a very low fatality rate in patients.” (Million et al., 2020)
- Borsche et al. (2021)
- In the Title: COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3
- In the abstract: “The two datasets provide strong evidence that low D3 is a predictor rather than a side effect of the infection. Despite ongoing vaccinations, we recommend raising serum 25(OH)D levels to above 50 ng/ml to prevent or mitigate new outbreaks due to escape mutations or decreasing antibody activity.”
- In the conclusion: “the authors strongly recommend combining vaccination with routine strengthening of the immune system of the whole population by vitamin D3 supplementation to consistently guarantee blood levels above 50 ng/ml (125 nmol/l). From a medical point of view, this will not only save many lives but also increase the success of vaccination. From a social and political point of view, it will lower the need for further contact restrictions and lockdowns. From an economical point of view, it will save billions of dollars worldwide, as vitamin D3 is inexpensive and – together with vaccines– provides a good opportunity to get the spread of SARS‐CoV‐2 under control.”[NOTE: Including this quote addressing the administration of Vitamin D in “combination to the vaccine” does not reflect an endorsement of the vaccine from my end. Given the evidence provided in this document, I do not endorse the administration of the vaccine under any circumstances, or any age group].
- In the Title: COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3
- “A meta-analysis study reported that music can modulate cytokine levels (including reducing IL-6 levels [IL-6 is one of the major inflammatory cytokines implicated in COVID-19]), as well as neuroendocrine-immune responses triggered by stress, including physical stress caused by viral infection (Fancourt et al., 2014).” [Comment: Given the therapeutic value of music (in the same way that games can help in diseases such as Alzheimer’s), including through an anti-inflammatory response, why are simpler, safer methods of addressing COVID-19 ignored in favor of questionable treatments?]
- There appears to be a concerted antagonistic effort in the medical field (often in letters, and not peer reviewed articles, to the editor of medical journals) towards the potential efficacy of ivermectin in the treatment of COVID-19 (e.g. Temple et al., 2021). Part of the efforts seem directed/focused on highlighting the side effects of ivermectin. Below is data extracted from the WHO adverse event website VigiAccess™ (http://vigiaccess.org); data accessed 10/26/21. Keep in mind that ivermectin was approved for medical use in 1981, while the COVID-19 vaccines were “approved” in late 2020.
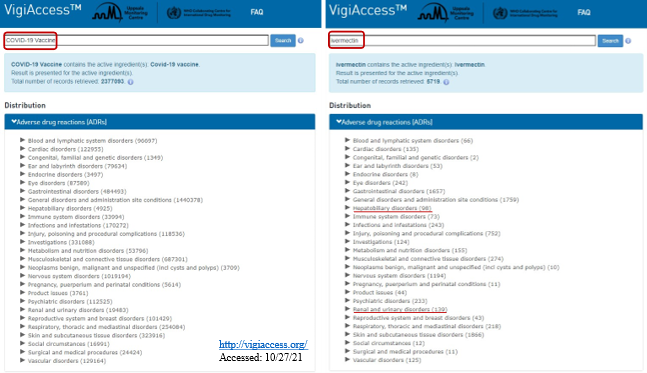
Figure 14: Comparison of COVID-19 vaccine adverse events relative to ivermectin
- Various treatments and protocols are available to address the effects of SARS-CoV-2 and the resulting COVID-19. Some of these are addressed below. Some of what is addressed below is common sense treatments that have either been used in medicine for a long time for other disorders that cause similar symptoms e.g. asthma, or potentially known for centuries (e.g. topical saline (i.e. nasal sprays in this case) to reduce microbial burden). However, also refer to McCullough et al. (2020) and see diagram below. (Further information available at: https://www.truthforhealth.org/)
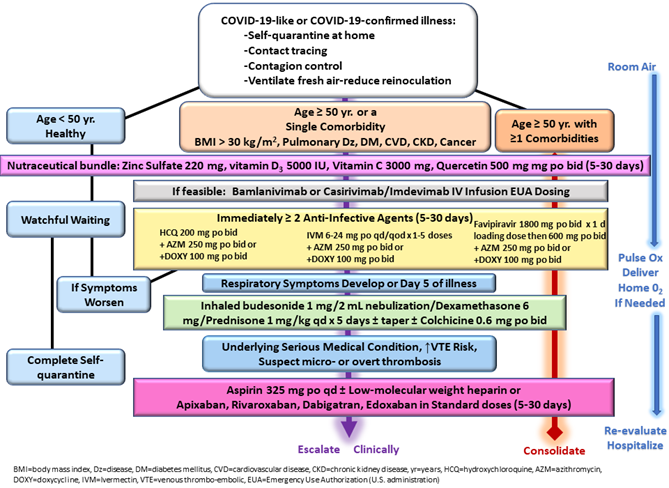
Figure 15: “Fig. 3. Sequential multidrug treatment algorithm for ambulatory acute COVID-19 like and confirmed COVID-19 illness in patients in self-quarantine. Yr = year, BMI = body mass index, Dz = disease, DM = diabetes mellitus, CVD = cardiovascular disease, chronic kidney disease, HCQ = hydroxychloroquine, IVM = ivermectin, Mgt = management, Ox = oximetry, reproduced with permission from reference.” (McCullough et al., 2020)
- “A recent meta-analysis (Kohler et al., 2018) of studies conducted in individuals with major depressive disorder following antidepressant treatment, mostly including selective serotonin reuptake inhibitors (SSRIs), supports that, overall, antidepressants may be associated with decreased plasma levels of 4 of 16 tested inflammatory mediators, including IL-10, TNF-α, and CCL-2, which are associated with COVID-19 severity (Hojyo et al., 2020), as well as IL-6, which is highly correlated with disease mortality (Hojyo et al., 2020;Ye et al., 2020)… In this multicenter observational retrospective study, antidepressant use at usual antidepressant doses was significantly and substantially associated with lower risk of intubation or death among adult patients hospitalized for COVID-19.” (Hoertel et al., 2021).
- “Results: The results revealed a reduction in frequency and length of hospitalization, in need of non-invasive oxygen therapy, in progression to intensive care units and in number of deaths. The results also confirmed the very high safety profile of quercetin and suggested possible anti-fatigue and pro-appetite properties. Conclusion: QP [quercetin] is a safe agent and in combination with standard care, when used in early stage of viral infection, could aid in improving the early symptoms and help in preventing the severity of COVID-19 disease… Quercetin is characterized by three crucial properties: antioxidant, anti-inflammatory and immunomodulatory.” (Di Pierro et al., 2021a)
- “QP [quercetin] statistically shortens the timing of molecular test conversion from positive to negative, reducing at the same time symptoms severity and negative predictors of COVID-19.” (Di Pierro et al., 2021b)
- Arefin (2021) recommends the use of Povidone Iodine (PVP-I) oro-nasal spray as a shield against COVID-19, a “strong microbicidal agent having 99.99% virucidal efficacy in its only 0.23% concentration, irrespective of all known viruses, even in SARS- CoV-2 (in vitro).” [NOTE: the potency of PVP-I is well known in the medical field. The author does indicate that “oral PVP-I, throat spray, nasal spray formulations are currently available as over-the-counter medications in many countries”. My concern in this case would potentially be about potential effects on the thyroid (please also see Guenezan et al. (2021) in this section). The author does warn about contraindications in patients with “iodine allergy or those undergoing radioiodine treatment or thyroid dysfunction”; Paper is also not very well written]
- Guenezan et al. (2021) state that “Nasopharyngeal decolonization may reduce the carriage of infectious SARS-CoV-2 in adults with mild to moderate COVID-19. Thyroid dysfunction occurred in 42% of the patients exposed to PI [Povidone-Iodine], with spontaneous resolution upon treatment discontinuation, as previously reported.”
- “…in human airway-derived cell models, moxidectin and ivermectin failed to inhibit SARS-CoV-2 infection…these findings suggest that, even by using a high-dose regimen of ivermectin or switching to another drug in the same class are unlikely to be useful for treatment against SARS-CoV-2 in humans.” (Dinesh Kumar et al., 2021) [NOTE: however, there are limitations to this study: conducted in vitro; does not take into consideration what has been reported clinically – see https://ivmmeta.com/ – for ongoing analysis relating to – Ivermectin]
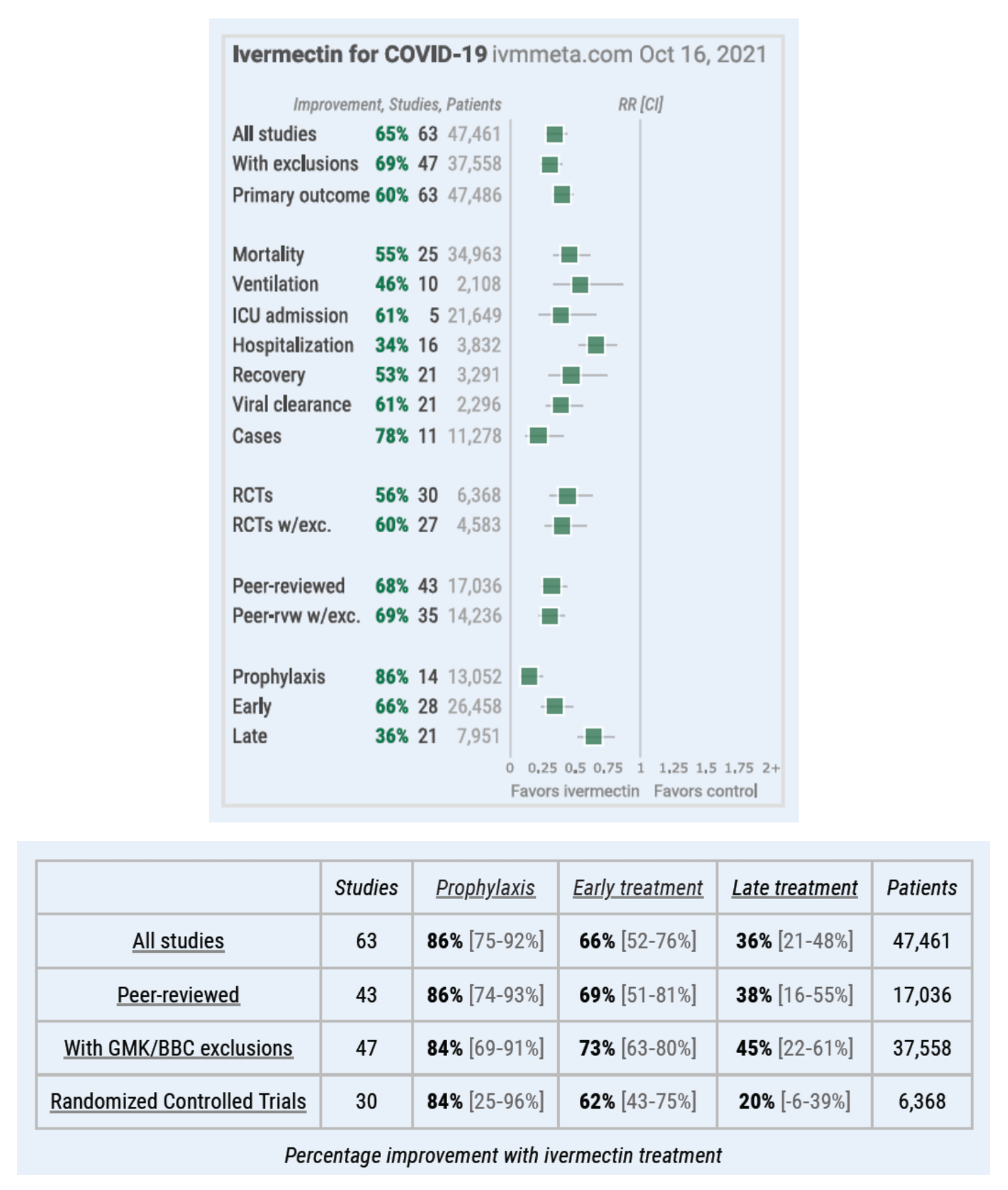
Figure 16: Ivermectin for COVID-19: real-time meta analysis of 63 studies Covid Analysis, Oct 16, 2021 [date of extraction], Version 133— removed Niaee [BBC, GMK response] https://ivmmeta.com/
- Expert Review Report by Jacques Descotes MD, PharmD, PhD, Professor Emeritus, Claude Bernard University of Lyon Fellow, US Academy of Toxicological Sciences Eurotox Registered Toxicologist: “Hundreds of millions of human subjects have been treated with ivermectin for curative or prophylactic purposes worldwide over the last 3 decades. The reference list of this report demonstrates that a large body of data is available, which allows for a detailed analysis of ivermectin medical safety. Undoubtedly, uncertainties remain regarding ivermectin pharmacological effects and mechanisms of action, but when removed, this is not anticipated to alter the main conclusions of this report in any significant way as they rely on an extensive and consistent body of medical publications. Taking into account all the above, the author of the present analysis of the available medical data concludes that the safety profile of ivermectin has so far been excellent in the majority of treated human patients so that ivermectin human toxicity cannot be claimed to be a serious cause for concern.” (Descotes, 2021)
- “In patients with mild and moderate COVID-19, a single oral administration of Ivermectin did not significantly increase either the negativity of RT-PCR or decline in viral load at day 5 of enrolment compared with placebo.” (Mohan et al., 2021) [NOTE: It is questionable whether the dose the authors report is even therapeutic i.e. it is possible the dose administered is subtherapeutic. Authors report the administration of a single dose of 24 or 12 mg. However, McCullough et al. (2020) suggests “200-600 mcg/kg [6-36 mg] single oral dose given daily or every other day for 2-3 administrations”. – note how weight is considered in the dosing and more than one dose appears to be required.]
- “Findings: In an observational cohort study of 412 adult patients with COVID-19, aspirin use was associated with a significantly lower rate of mechanical ventilation, intensive care unit (ICU) admission, and in-hospital mortality after controlling for confounding variables. Meaning: Aspirin may have lung-protective effects and reduce the need for mechanical ventilation, ICU admission, and in-hospital mortality in hospitalized COVID-19 patients.” (Chow et al., 2021)
- “The pharmacology of anti-SARS-CoV-2 drugs, Molnupiravir (M) and repurposed Ivermectin (IV) were compared. The IC50 for the inhibition of viral replication were 0.3μM for M and 2.8μM for IV. Both drugs have good oral absorption, with M achieving peak plasma concentrations by 2 hours and IV by 5 hours. The plasma half life were 7 hours for M and 81-91 hours for IV. M inhibits viral replication inducing viral mutagenesis in RdRp, causing viral error catastrophe and viral extinction. IV affects viral cell entry, nuclear transport and inhibits replication via RdRp. IV has additional effect to suppress cytokine production through STAT-3 inhibition. M is a more potent antiviral drug and IV has a longer residence in the body.” (AAL, 2021)
- “Our results show that therapeutic and prophylactic administration of EIDD-2801-an oral broad-spectrum antiviral agent that is currently in phase II/III clinical trials-markedly inhibited SARS-CoV-2 replication in vivo, and thus has considerable potential for the prevention and treatment of COVID-19.” (Wahl et al., 2021)
- “Ivermectin was found as a blocker of viral replicase, protease and human TMPRSS2, which could be the biophysical basis behind its antiviral efficiency” [in silico investigation] (Choudhury et al., 2021)
- “Hypertonic nasal saline, which facilitates mucociliary clearance, likely decreases viral burden through physical removal. Other additives, such as povidone-iodine, may aid in eliminating viral particles within the nasal cavity and nasopharynx prior to active infection. Given available evidence, saline irrigations with or without indicated additives may be safe to use in the presence of COVID-19.”(Farrell et al., 2020)
- “INCS [Intranasal Corticosteroid] therapy is associated with a lower risk for COVID-19-related hospitalization, ICU admission, or death.” (Strauss et al., 2021)
- “…we determined that melatonin usage was associated with a reduced likelihood of SARS-CoV-2 positive test result compared to use of angiotensin II receptor blockers (OR = 0.70, 95% CI 0.54-0.92) or angiotensin-converting enzyme inhibitors (OR = 0.69, 95% CI 0.52-0.90). Importantly, melatonin usage (OR = 0.48, 95% CI 0.31-0.75) is associated with a 52% reduced likelihood of a positive laboratory test result for SARS-CoV-2 in African Americans after adjusting for age, sex, race, smoking history, and various disease comorbidities…In summary, this study presents an integrative network medicine platform for predicting disease manifestations associated with COVID-19 and identifying melatonin for potential prevention and treatment of COVID-19.” (Zhou et al., 2020b)
- Not related to COVID-19 but addressing the treatment of various factors that manifest themselves in COVID-19 – “Melatonin, alongside its traditionally accepted role as the master hormonal regulator of the circadian rhythm, is a promising adjunctive drug for sepsis through its anti-inflammatory, antiapoptotic and powerful antioxidant properties.”(Colunga Biancatelli et al., 2020)
- “Melatonin is readily available, can be easily synthesized in large quantities, is inexpensive, has a very high safety profile and can be easily self-administered. Melatonin is endogenously-produced molecule in small amounts with its production diminishing with increased age. Under the current critical conditions, large doses of melatonin alone or in combination with currently-recommended drugs, e.g., hydroxychloroquine/chloroquine, to resist COVID-19 infection would seem judicious.”(Reiter et al., 2020)
- Remdesivir:
- Prior to addressing some literature pertaining to remdesivir, it is important to take note of the comparison of reported side effects relative to ivermectin. This is data from the WHO VigiAccess™ database (http://www.vigiaccess.org/). The concern pertaining to safety are also outlined by (Gerard et al., 2021)
- Prior to addressing some literature pertaining to remdesivir, it is important to take note of the comparison of reported side effects relative to ivermectin. This is data from the WHO VigiAccess™ database (http://www.vigiaccess.org/). The concern pertaining to safety are also outlined by (Gerard et al., 2021)
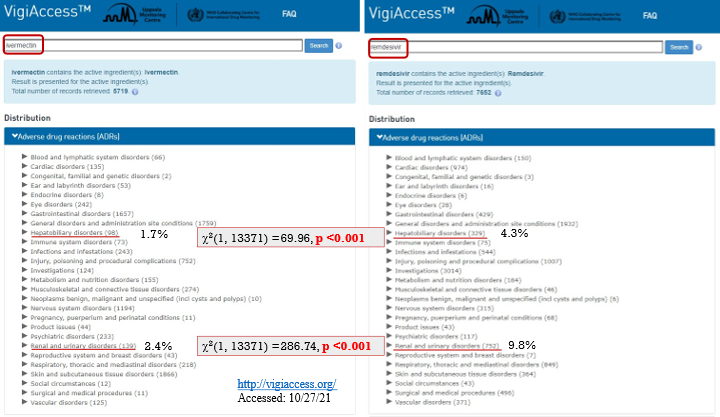
Figure 17: Statistical analysis indicates that the proportion of reports for remdesivir are significantly (p<0.001) higher than those of ivermectin for Hepatobiliary disorders and Renal and Urinary disorders.
- Remdesivir continued:
- Additionally, the concern pertaining to safety, most especially pertaining to its negative effects on the kidneys that could ultimately impact survival, are of great concern and also outlined in the scientific literature (Rahimi et al., 2020; Chouchana et al., 2021; Gerard et al., 2021; Silva et al., 2021).
- “Versus hydroxychloroquine, lopinavir/ritonavir, or tocilizumab, the use of remdesivir was associated with an increased chance of reporting renal and urinary disorders regardless of gender and age of patients (2.53; 95%CI: 2.10-3.06). The ROR [reporting odds ratios] remained significant when we restricted the analysis to hydroxychloroquine (4.31; 95%CI: 3.25-5.71) or tocilizumab (3.92; 95%CI: 2.51-6.12). Our results reinforce this already reported signal, emphasizing that it could be extremely useful for health professionals who prescribe this new antiviral to treat COVID-19, mainly knowing its low efficacy.” (Silva et al., 2021)
- “Our findings, based on postmarketing real-life data from >5000 COVID-19 patients, support that kidney disorders, almost exclusively AKI [acute kidney injury], represent a serious, early, and potentially fatal adverse drug reaction of remdesivir” (Chouchana et al., 2021)
- “Remdesivir solution is administered with a cyclodextrin carrier that filters solely by the glomeruli; thereby patients with abnormal renal function cannot eliminate it quickly; therefore, remdesivir can lead to renal failure or liver dysfunction during therapeutic process of COVID-19.” (Rahimi et al., 2020)
- “Versus hydroxychloroquine, lopinavir/ritonavir, or tocilizumab, the use of remdesivir was associated with an increased chance of reporting renal and urinary disorders regardless of gender and age of patients (2.53; 95%CI: 2.10-3.06). The ROR [reporting odds ratios] remained significant when we restricted the analysis to hydroxychloroquine (4.31; 95%CI: 3.25-5.71) or tocilizumab (3.92; 95%CI: 2.51-6.12). Our results reinforce this already reported signal, emphasizing that it could be extremely useful for health professionals who prescribe this new antiviral to treat COVID-19, mainly knowing its low efficacy.” (Silva et al., 2021)
- Ader et al. (2021) state that “Together with previous evidence, results from the DisCoVeRy trial do not support the use of remdesivir in hospitalised patients with COVID-19 in a population with symptoms for more than a week and requiring oxygen support.”
- Other studies have reported contrary findings. In a comparison between a 5-day course vs 10-day course of remdesivir 64% of patients treated were reported to have recovered in the 5-day group relative to 54% of patients in the 10-day group. However, “In patients with severe Covid-19 not requiring mechanical ventilation, our trial did not show a significant difference between a 5-day course and a 10-day course of remdesivir. With no placebo control, however, the magnitude of benefit cannot be determined.” (Goldman et al., 2020)1
- “Our data show that remdesivir was superior to placebo in shortening the time to recovery in adults who were hospitalized with Covid-19 and had evidence of lower respiratory tract infection.” (Beigel et al., 2020)1
- “In pre-clinical models, remdesivir has demonstrated potent antiviral activity against diverse human and zoonotic b-coronaviruses, including SARS-CoV-2.” (Jorgensen et al., 2020)
- Some studies have also reported faster recovery times with remdesivir treatment but little change in mortality rates (Jorgensen et al., 2020; Singh et al., 2020)
- Additionally, the concern pertaining to safety, most especially pertaining to its negative effects on the kidneys that could ultimately impact survival, are of great concern and also outlined in the scientific literature (Rahimi et al., 2020; Chouchana et al., 2021; Gerard et al., 2021; Silva et al., 2021).
- Chloroquine (CQ) and hydroxychloroquine (HCQ) alone or in combination therapy with other treatments (McCullough et al., 2020)
- “Precious time is squandered with a “wait and see” approach in which there is no anti-viral treatment as the condition worsens, possibly resulting in unnecessary hospitalization, morbidity, and death.” (McCullough et al., 2020)
- “…treatment with hydroxychloroquine alone and in combination with azithromycin was associated with reduction in COVID-19 associated mortality.” (Arshad et al., 2020)
- “HCQ, which is three times more potent than CQ in SARS-CoV-2 infected cells (EC50 0.72 μM), was significantly associated with viral load reduction/disappearance in COVID-19 patients compared to controls.” (Klimke et al., 2020)
- “Our findings reveal that remdesivir [NOTE: See other comments regarding the dangers of kidney failure associated with this drug] and chloroquine are highly effective in the control of 2019-nCoV infection in vitro. Since these compounds have been used in human patients with a safety track record and shown to be effective against various ailments, we suggest that they should be assessed in human patients suffering from the novel coronavirus disease.” (Wang et al., 2020)
- “…several studies have shown the effectiveness of this molecule, including against coronaviruses among which is the severe acute respiratory syndrome (SARS)-associated coronavirus ….[clinical trials] showed that chloroquine could reduce the length of hospital stay and improve the evolution of COVID-19 pneumonia, leading to recommend the administration of 500 mg of chloroquine twice a day in patients with mild, moderate and severe forms of COVID-19 pneumonia.” (Colson et al., 2020)
- “Our review shows that SARS-Cov-2 selectively induces a high level of IL-6 and results in the exhaustion of lymphocytes. The current evidence indicates that tocilizumab, an IL-6 inhibitor, is relatively effective and safe.” (Tang et al., 2020)
- “Chloroquine phosphate, an old drug for treatment of malaria, is shown to have apparent efficacy and acceptable safety against COVID-19 associated pneumonia in multicenter clinical trials conducted in China.” (Gao et al., 2020)
- “Chloroquine enhanced zinc uptake… The combination of chloroquine with zinc enhanced chloroquine’s cytotoxicity and induced apoptosis in A2780 cells” (Xue et al., 2014)
- “Chloroquine is effective in preventing the spread of SARS CoV in cell culture. Favorable inhibition of virus spread was observed when the cells were either treated with chloroquine prior to or after SARS CoV infection.” (Vincent et al., 2005)
- “Ivermectin is an FDA-approved broad-spectrum antiparasitic agent with demonstrated antiviral activity against a number of DNA and RNA viruses, including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).” (Formiga et al., 2021)
- Discovered in the late 70’s ivermectin, it was “Originally introduced as a veterinary drug, it kills a wide range of internal and external parasites in commercial livestock and companion animals. It was quickly discovered to be ideal in combating two of the world’s most devastating and disfiguring diseases which have plagued the world’s poor throughout the tropics for centuries. It is now being used free-of-charge as the sole tool in campaigns to eliminate both diseases globally. It has also been used to successfully overcome several other human diseases and new uses for it are continually being found.” (Crump and Omura, 2011)
- “Ivermectin treatment was associated with lower mortality during treatment of COVID-19, especially in patients with severe pulmonary involvement” (Rajter et al., 2021)
- “Here, we show that countries with routine mass drug administration of prophylactic chemotherapy including ivermectin have a significantly lower incidence of COVID-19.” (Hellwig and Maia, 2021)
- Re: ivermectin – “The consistency of positive results across a wide variety of cases has been remarkable. It is extremely unlikely that the observed results could have occurred by chance” (Zaidi and Dehgani-Mobaraki, 2021)
- “Statistically significant improvements are seen for mortality, hospitalization, recovery, cases, and viral clearance. 29 studies show statistically significant improvements in isolation.” (ivmmeta.com, 2021)
- “Excitingly, cell culture experiments show robust antiviral action [by ivermectin] towards HIV-1, dengue virus (DENV), Zika virus, West Nile virus, Venezuelan equine encephalitis virus, Chikungunya virus, Pseudorabies virus, adenovirus, and SARS-CoV-2 (COVID-19).” (Jans and Wagstaff, 2020)
- “Ivermectin can be a potential molecule for prophylaxis and treatment of people infected with Coronavirus, owing to its anti-viral properties coupled with effective cost, availability and good tolerability and safety.” (Vora et al., 2020)
- “Ivermectin plays a role in several biological mechanisms, therefore it could serve as a potential candidate in the treatment of a wide range of viruses including COVID-19 as well as other types of positive-sense single-stranded RNA viruses. In vivo studies of animal models revealed a broad range of antiviral effects of ivermectin, however, clinical trials are necessary to appraise the potential efficacy of ivermectin in clinical setting” (Heidary and Gharebaghi, 2020)
- “We report here that Ivermectin, an FDA-approved anti-parasitic previously shown to have broad-spectrum anti-viral activity in vitro, is an inhibitor of the causative virus (SARS-CoV-2), with a single addition to Vero-hSLAM cells 2 h post infection with SARS-CoV-2 able to effect ~5000-fold reduction in viral RNA at 48 h” (Caly et al., 2020)
- “Ivermectin exerts broad-spectrum antiviral activity against several animal and human viruses, including both RNA and DNA viruses” (Sharun et al., 2020)
- “…the authors found Ivermectin-Doxycycline combination therapy had a better success of symptomatic relief; shortened recovery duration, reduced adverse effects, and superior patient compliance compared to the Hydroxychloroquine-Azithromycin combination. The authors concluded ivermectin as a better choice for the treatment of patients with mild to moderate COVID-19 disease (Chowdhury et al., 2021)” (Pandey et al., 2020)
- “Meta-analysis of 15 trials found that ivermectin reduced risk of death compared with no ivermectin…ivermectin prophylaxis reduced COVID-19 infection by an average 86% (Bryant et al., 2021)” (Bilezikian et al., 2020)
- “Ivermectin (IVM) is one of the best known and most widely used antiparasitic drugs in human and veterinary medicine…IVM has been shown to regulate glucose and cholesterol levels in diabetic mice [1], to suppress malignant cell proliferation in various cancers [2], to inhibit viral replication in several flaviviruses [3], and to reduce survival in major insect vectors of malaria and trypanosomiasis [4,5].” (Laing et al., 2017)
- “Ivermectin is an antiparasitic drug with a broad spectrum of activity, high efficacy as well as a wide margin of safety” (Gonzalez Canga et al., 2008)
- “This study demonstrated that ivermectin is generally well tolerated at these higher doses and more frequent regimens.” (Guzzo et al., 2002)
- Other factors that assist (e.g. Vitamin D, diet)
- Lai et al. (2021) [NOTE: This paper is not the best of quality however, it ultimately points to the reality of the importance of appropriate nutrition and of the micronutrients addressed, which have been documented in various other papers, COVID-19- and non-COVID-19-related]:
- “The relationship between Vit A and infection is its role in mucosal epithelium integrity (skin and mucous membrane), the supplementation could be an option for assisted-treating the SARS-CoV-2 virus and a possible prevention of lung infection.”
- “Vit C/ascorbic acid stimulates oxygen radical scavenging activity of the skin and enhances epithelial barrier function. Ascorbic acid alone or with other natural compounds (baicalin and theaflavin) may inhibit the expression of angiotensin-converting enzyme II in human small alveolar epithelial cells and limited the entry of SARS-CoV-2.”
- “Vitamin D receptors can be expressed by immune cells, and different immune cells (macrophages, monocytes, dendritic cells, T cells, and B cells) can convert Vit D into its active form 1,25-(OH)2 D. Oral vitamin D intake can be a readily way to restrict the viral infection through downregulation of ACE2 receptor and to attenuate the disease severity by decreasing the frequency of cytokine storm and pulmonary pro-inflammatory response.”
- “Vit E supports T-cell mediated functions, optimization of Th1 response, and suppression of Th2 response. Vitamin E supplementation can lower the production of superoxides and may favors the antioxidants and benefit the progress of COVID-19 treatment.”
- “Zinc plays an essential role in both innate and adaptive immune systems and cytokine production, and Zinc-dependent viral enzymes to initiate the infectious process have proved the Zinc levels are directly associated with symptoms relieved of COVID-19.”
- “Iron is an essential component of enzymes involved in the activation of immune cells, lower iron levels predispose to severe symptoms of SARS-CoV-2, and monitoring the status can predict the disease severity and mortality.”
- “Selenium participates in the adaptive immune response by supporting antibody production and development. Deficiency can reduce antibody concentration, decreased cytotoxicity of NK cells, compromised cellular immunity, and an attenuated response to vaccination.”
- The authors conclude that “Micronutrients are involved in immunity from the virus entering the human to innate immune response and adaptive immune response. Micronutrients are indispensable in immune response of vaccination.” [NOTE: Strange how the micronutrients are not addressed as being indispensable in the natural immune response.]
- “The relationship between Vit A and infection is its role in mucosal epithelium integrity (skin and mucous membrane), the supplementation could be an option for assisted-treating the SARS-CoV-2 virus and a possible prevention of lung infection.”
- “Vitamin D deficiency significantly correlates with the severity of SARS-CoV-2 infection…Active forms of vitamin D and lumisterol can inhibit SARS-CoV-2 replication machinery enzymes, which indicates that novel vitamin D and lumisterol metabolites are candidates for antiviral drug research.” (Qayyum et al., 2021)
- “Among hospitalized COVID-19 patients, pre-infection deficiency of vitamin D was associated with increased disease severity and mortality” (Dror et al., 2021)
- “There is growing evidence that vitamin D signaling is active throughout the immune system, and that it is physiologically important in protecting the human host from bacterial and viral invaders… Many clinical reports suggest that vitamin D supplementation, at least for the elderly and patients with low 25D status, can help in protecting against COVID-19 infection and severe course of disease.” (Ismailova and White, 2021)
- “In conclusion, low serum 25 (OH) Vitamin-D level was significantly associated with a higher risk of COVID-19 infection. The limited currently available data suggest that sufficient Vitamin D level in serum is associated with a significantly decreased risk of COVID-19 infection.” (Teshome et al., 2021)
- “We found a markedly high prevalence (100%) of hypovitaminosis D in patients admitted to hospital with COVID-19, suggesting a possible role of low vitamin D status in increasing the risk of SARS-CoV-2 infection and subsequent hospitalization. The inverse association between serum 25(OH)D levels and risk of in-hospital mortality observed in our cohort suggests that a lower vitamin D status upon admission may represent a modifiable and independent risk factor for poor prognosis in COVID-19.” (Infante et al., 2021)
- “Among patients hospitalized with COVID-19, treatment with calcifediol [25-hydroxyvitamin D3), compared with those not receiving calcifediol, was significantly associated with lower in-hospital mortality during the first 30 days.” (Alcala-Diaz et al., 2021)
- “…calcifediol treatment on ICU admission…showed that treated patients had a reduced risk to require ICU. Overall mortality was 10%. In the Intention-to-Treat analysis, 21 (4.7%) out of 447 patients treated with calcifediol at admission died compared to 62 patients (15.9%) out of 391 non-treated.” (Nogues et al., 2021) [NOTE: currently listed by Retraction Watch as Retracted/Withdrawn]
- “Vitamin D supplementation might be associated with improved clinical outcomes, especially when administered after the diagnosis of COVID-19.” (Pal et al., 2021)
- “A 5000 IU daily oral vitamin D3 supplementation for 2 weeks reduces the time to recovery for cough and gustatory sensory loss among patients with sub-optimal vitamin D status and mild to moderate COVID-19 symptoms. The use of 5000 IU vitamin D3 as an adjuvant therapy for COVID-19 patients with suboptimal vitamin D status, even for a short duration, is recommended” (Sabico et al., 2021)
- “Therapeutic improvement in vitamin D to 80–100 ng/ml has significantly reduced the inflammatory markers associated with COVID-19 without any side effects.” (Lakkireddy et al., 2021)
- “Fourteen observational studies offer evidence that serum 25-hydroxyvitamin D concentrations are inversely correlated with the incidence or severity of COVID-19. The evidence to date generally satisfies Hill’s criteria for causality in a biological system, namely, strength of association, consistency, temporality, biological gradient, plausibility (e.g., mechanisms), and coherence, although experimental verification is lacking. Thus, the evidence seems strong enough that people and physicians can use or recommend vitamin D supplements to prevent or treat COVID-19 in light of their safety and wide therapeutic window.” (Mercola et al., 2020)
- “Nevertheless, recent publications consistently show a higher prevalence of vitamin D deficiency in patients presenting with severe forms of COVID-19 (Grant et al., 2020)” (Bilezikian et al., 2020)
- “Through several mechanisms, vitamin D can reduce risk of infections. Those mechanisms include inducing cathelicidins and defensins that can lower viral replication rates and reducing concentrations of pro-inflammatory cytokines that produce the inflammation that injures the lining of the lungs, leading to pneumonia, as well as increasing concentrations of anti-inflammatory cytokines.” (Bilezikian et al., 2020)
- “Several studies demonstrated the role of vitamin D in reducing the risk of acute viral respiratory tract infections and pneumonia. These include direct inhibition with viral replication or with anti-inflammatory or immunomodulatory ways. In the meta-analysis, vitamin D supplementation has been shown as safe and effective against acute respiratory tract infections.” (Ali, 2020)
- “In this review, inflammation associated with pre-existing comorbidities was highlighted as a significant risk factor for COVID-19 patients…Nutrients such as vitamin C, vitamin D, and zinc may hold some promise for the treatment of COVID-19. Likewise, nutrients with anti-inflammatory, antithrombotic, and antioxidant properties may prevent or attenuate the inflammatory and vascular manifestations associated with COVID-19. Indeed, following healthy dietary patterns and avoiding unhealthy dietary patterns, such as the Mediterranean and Western diets, respectively, may have beneficial effects against infection but require significantly more research. Our primary conclusion is that it is vitally important to maintain a healthy diet and lifestyle during the pandemic.” (Zabetakis et al., 2020)
- “Our pilot study demonstrated that administration of a high dose of Calcifediol or 25-hydroxyvitamin D, a main metabolite of vitamin D endocrine system, significantly reduced the need for ICU treatment of patients requiring hospitalization due to proven COVID-19.” (Entrenas Castillo et al., 2020)
- “…increased mortality in vitamin D deficient COVID-19 patients. As per the flexible approach in the current COVID-19 pandemic authors recommend mass administration of vitamin D supplements to population at risk for COVID-19.” (Jain et al., 2020)
- “…treatment with cholecalciferol [vitamin D3] booster therapy, regardless of baseline serum 25(OH)D levels, appears to be associated with a reduced risk of mortality in acute in-patients admitted with COVID-19.” (Ling et al., 2020)
- “Based on many preclinical studies and observational data in humans, ARDS [Acute Respiratory Distress Syndrome – major complication of COVID-19] may be aggravated by vitamin D deficiency and tapered down by activation of the vitamin D receptor” (Quesada-Gomez et al., 2020)
- “A vitamin D / magnesium / vitamin B12 combination in older COVID-19 patients was associated with a significant reduction in the proportion of patients with clinical deterioration requiring oxygen support, intensive care support, or both. This study supports further larger randomized controlled trials to ascertain the full benefit of this combination in ameliorating the severity of COVID-19.” (Tan et al., 2020)
- “The National Academy of Medicine…recommends the rapid serum vitamin D (i.e. 25 OHD) testing in people over 60 years of age with Covid-19, and a loading dose of 50,000 to 100,000 IU in case of deficiency, which could help limit respiratory complications; recommends vitamin D supplementation of 800 to 1000 IU/day in people under 60, as soon as the diagnosis of Covid-19 is confirmed.” (French National Academy of Medicine, 2020)
- “We observed that Mediterranean diet adherence was negatively associated with both COVID-19 cases and related deaths across 17 regions in Spain and that the relationship remained when adjusted for factors of well-being. We also observed a negative association between Mediterranean diet adherence and COVID-19 related deaths across 23 countries when adjusted for factors of well-being and physical inactivity. The anti-inflammatory properties of the Mediterranean diet – likely due to the polyphenol content of the diet – may be a biological basis to explain our findings.” (Greene et al., 2021)
- Lai et al. (2021) [NOTE: This paper is not the best of quality however, it ultimately points to the reality of the importance of appropriate nutrition and of the micronutrients addressed, which have been documented in various other papers, COVID-19- and non-COVID-19-related]:
1 This paper involved research conducted using support from Gilead Sciences which is the developer of remdesivir. This is fully declared in the paper.
